CASE REPORT | https://doi.org/10.5005/jp-journals-10079-1041 |
Budding Well: A Fun and Sharing-based Rehabilitation Program through Music and Arts for the Children and Teenagers with Extremity Anomalies
1,9,10Department of Orthopaedics and Traumatology, Prince of Wales Hospital, Hong Kong
2Department of Rehabilitation Sciences, Hong Kong Polytechnic University, Hong Kong
3,5-7Department of Orthopaedics and Traumatology, Chinese University of Hong Kong, Shatin, Hong Kong
4Occupational Therapy Department, Prince of Wales Hospital, Hong Kong
8Department of Social Work, Chinese University of Hong Kong, Shatin, Hong Kong
Corresponding Author: Pak-Cheong Ho, Department of Orthopaedics and Traumatology, Prince of Wales Hospital, Hong Kong, Phone: +(852) 3505–2722, e–mail: pcho@ort.cuhk.edu.hk
ABSTRACT
Introduction: Children with physical disabilities are less likely to access music and arts due to their extremity anomalies. “Budding Well” is a non-conventional rehabilitation program providing music and arts courses for the targeted participants. The program has run through the third year and a review of the service outcomes has been sorted.
Materials and methods: Aged 6–18 years with different kinds and degrees of limb dysfunctions were invited to join the program. The course consisted of 10 learning classes on playing harmonica (music) or painting (arts). Functional assessments [Bruininks-Oseretsky-Test-of-Motor- Proficiency second edition (BOT-2) and Grip-and-pinch strength] and psychosocial centric questionnaires [Lyubomirsky and Lepper’s Subjective Happiness Scale (SHS), Well-being Index (WHO-5), and Culture-free Self-esteem Inventory-2 (CFESI-2) Form A] were performed and completed at the first and last (10th) class. Program evaluation questionnaire was filled at the last class.
Results: Thirty-five participants (male = 20, female = 15) of mean age 8.65 joined the program. Functional assessments and psychosocial centric questionnaire outcomes except CFESI-2 did not show any statistical difference. Age sensitivity testing in CFESI-2 Social domain score showed the best result when cut-off age was at 10.5 (p = 0.04) and this cut-off value was further proved by receiver operating characteristic (ROC) analysis (p < 0.01). On subjective evaluation, parents noticed a significant improvement in the hand function of their children (p= 0.01).
Conclusion: Hand functions and psychosocial skills of children and teenagers with different levels of physical disabilities or disfigurement proved to benefit from our program through music and arts. Participants of age at 10.5 best responded to the program, particularly on the significant improvement in self-esteem.
How to cite this article: Ho P-C, Wong JM-W, Chau W-W, et al. Budding Well: A Fun and Sharing-based Rehabilitation Program through Music and Arts for the Children and Teenagers with Extremity Anomalies. J Orth Joint Surg 2022;4(1):40–46.
Source of support: Nil
Conflict of interest: None
Keywords: Art, Child, Musculoskeletal abnormalities, Music, Rehabilitation
INTRODUCTION
Budding Well is a nonprofit making rehabilitation service program for children and teenagers with extremity anomalies through music and arts. It was established as a service outreach jointly organized by a tertiary institute and local hospital system since year 2016.1 The program composes of a team of orthopedic hand surgeons, occupational therapists, physiotherapists, and social workers. Early surgery to children with congenital upper limb deformities is commonly performed within the first 2 years of life. Surgery on limb deformities aims at recovering certain limb potential for growth and development. Early intervention (surgery) is important to improve psychological abilities when children grow up. Rehabilitation following the surgery is an integral and continuing part of the treatment program aiming at enhancing hand functions, often up to adolescence. Rehabilitation is, therefore, an essential component to manage limb anomalies to maximize the physical functions after surgery. Achieving optimal upper limb functions is of priority with the use of accurate assessment to define and derive both objective and subjective outcomes.
Limb deficiency or deformity in children can be congenital or acquired. The limb function development of the children is usually affected, leading to a marginal performance in their activities of daily living. For instance, a child with brachydactyly finds him/ her difficult to hold a large object due to the shortened fingers; whereas children with a hypoplastic thumb find it difficult to hold a pen to write on a piece of paper. The physical abnormalities not only restrict the functional development but also affect their self- confidence in getting along with peers as well as their self-esteem due to the unfavorable cosmesis of their limbs. While parents may expect improvements in their children’s hand functions and cosmesis through surgery and subsequent rehabilitation program, they may still feel stressed when they must spend extra time to take care of the children.
Extra-curriculum activities (thereafter “interest courses”), e.g., music and art courses are common for children and teenagers in the service region, however, those with physical disabilities or disfigurement (such as in burns) may not be able to access such kind of activities easily leading to limiting their exposures and their potential talents on music and arts. “Budding Well” provides the opportunities to let those in need to expose to music (harmonica), and arts (drawing and painting). Through tailor-made music and art courses, participants can exercise their affected upper limbs and improve their hand functions. The courses can also provide a friendly social environment for them to enjoy music and arts with others suffering from similar disabilities, enriching their artistic interest and cultural life. The participants can eventually benefit from developing self-confidence, self-esteem, and social skill and prepare themselves properly to integrate into society toward adulthood.
We choose to teach playing harmonica and painting for a couple of reasons. They do not cost much to the participants. Harmonica is light and therefore easy to carry around, and painting materials share the same advantage. Comparing to other musical instruments, harmonica does not require multiple and complicated finger motions to perform and thus reduces the difficulty and potential frustration for the beginners, especially on this group of physically disadvantageous kids. The upright posture of the upper limb when playing harmonica trains bimanual dexterity and eye–ear–hand coordination. Teachers with professional backgrounds and experience in teaching harmonica and painting for the disabled lead the groups. When children are enjoying playing harmonica and painting, the escorting parents/legal guardians or caretakers share their experiences on taking care of the children at the same venue. Sharing the feelings among parents/legal guardians or caretakers are very useful to let them express their feeling comfortably thereafter to sort out certain difficulties through mutual support and encouragements.
Hand functions, self-esteem, happiness, and subjective well-being were monitored along with the extra-curriculum activities through different kinds of assessments. In this retrospective study, we aim at identifying the rehabilitation outcome after participating in the harmonica and painting courses, and the future direction of the service group development.
MATERIALS AND METHODS
Participants
Participants aged between 6 years and 18 years were recruited from a specialized orthopedic clinic from year 2016 to 2019. Ethics approval was obtained from a local ethics review committee (Reference Number: 2020.389). Informed consent was obtained from the parents or legal guardians of the participants. They had different conditions over their upper and/or lower limbs with varying degree of functional impairments. The “Budding Well” program was introduced to the potential clients and their parents/ legal guardians identified by the attending doctors at clinic visit. Children who were happy to join the program became members of the program. Each member was required to complete an application form which included ethical statements on data protection, and the use of information from assessments and questionnaires for data analysis and reporting results to the funder. Application forms were signed by the parents/legal guardians. Ethical approval was exempted being not initially designed as a research project. Interest courses were fully subsidized for members. All participants were able to comprehend, write and follow the instructions during the assessment. Hand function assessments as well as self-rated reports and inventory were conducted by occupational therapists before and after the courses.
Interest Courses
Both harmonica and art courses were carried out three times (terms) a year. Each term lasted for 3 months with 1–2 months apart. There were 10 classes in a term. Each class was directed by experienced trainers and lasted for 1.5 hours. Both courses were held in two separate rooms in the same site in the hospital on the same day. Functional assessments and psychosocial centric questionnaires were performed and completed by a dedicated experienced occupational therapist at the first and last (10th) classes.
Functional Assessments
In the functional aspect, Bruininks-Oseretsky Test of Motor Proficiency, Second Edition (BOT-2) is used to assess participants’ hand dexterity when Jamar dynamometer and pinch gauge are used for grip and pinch power assessment.
Bruininks-Oseretsky Test of Motor Proficiency, Second Edition: BOT-2 is an individually administered test that uses engaging, goal- directed activities to measure a wide array of hand manipulation skills in individuals aged 4 through 21.2,4 It is designed to provide rehabilitation professionals including occupational therapists, physiotherapists, physical education teachers, and researchers a reliable and efficient measure of fine and gross motor control skills. The test consists of eight subtests, including fine motor precision, fine motor integration, manual dexterity, bilateral coordination, balance, running speed and agility, upper-limb coordination, and strength.
In our data collection, we conducted the subtest “manual dexterity” which requires participants to reach, grasp, and manipulate small objects through bimanual coordination in the goal-directed activities. Activity items include picking up plastic pennies and placing them into a box, stringing small blocks, sorting cars, and placing pets into a pegboard. Participants’ performances in every activity are timed and the accuracy counted. After completing the assessment, total and mean scores were calculated (the higher scores the better motor skills).
Grip and pinch strength is the most commonly evaluated function of the hand as the measurements’ result reflect overall hand function and grip strength, an indicator of general health.5 In our data collection, Jamar hydraulic hand dynamometer is used to measure grip strength, which has established validity and reliability for grip strength assessment. It is also a criterion standard for measuring hand strength.6,11 In measuring pinch strength, B&L Engineering pinch gauge12 is used to measure pinch strength (lateral pinch, chuck pinch, and tip pinch). Studies found that the B&L Engineering pinch gauge has high calibration accuracy.12,13 The first position of the Jamar dynamometer is used during the measurement, and participants are instructed to follow the standard measurement position during the two assessments.
Psychosocial Centric Questionnaires
Several questionnaires were used to assess the functional ability and psychosocial characteristics of the participants. They completed the questionnaires before and after the course. The questionnaires included:
Lyubomirsky and Lepper’s Subjective Happiness Scale (SHS).14 It is a 4-items self-rated inventory. It is a global subjective measurement of whether the respondent is happy or an unhappy person. The scale consists of multiple items: two items ask respondents to characterize themselves using both absolute ratings and ratings relative to peers, while the other two ask respondents the extent to which each characterization describes them. This self-reported scale shows excellent psychometric properties with good construct validity and high internal consistency as well as reliability over time.15
Well-being Index (WHO-5).16 It is a short and generic global rating scale measuring subjective well-being. The questionnaire covers five positively worded items, related to positive mood (good spirits, relaxation), vitality (being active and waking up fresh and rested), and general interests (being interested in things). Respondents were asked to rate how well each of the five statements applied to him or her when considering the last 14 days. The scale has adequate validity both as a screening tool for depression and as an outcome measure in clinical trials and has been applied successfully across a wide range of study fields.
Culture-free Self-esteem Inventory-2 (CFESI-2) Form A.17 It is a self-rating inventory commonly used to measure self-esteem for clinical and research purposes. It aims to identify individuals who may need psychological assistance. Form A is intended for use with children in grades 3–9 providing a measure of general self-worth as well as more specific components of self-esteem related to peers, school, and the home. It contains a Lie Scale signifying the extent of defensiveness. A total score as well as four domains (general, social, academic, and parental) were calculated, where a lower score indicated lower self-esteem. Possessing a carefully developed construct, and satisfactory psychometric properties and easy administration, CFSEI Form A second edition is one of the widely used inventory by local researchers and practitioners.
Course Evaluation Questionnaire
A tailor-made course evaluation questionnaire was distributed to participants and parents after finishing the last (10th) class. The questionnaire comprised five questions asking for the following (1) the feeling after coming through the program (2) willingness to use their hands to handle daily activities (3) participating in different social activities (4) improving hand function, and (5) improving self-confidence. The answers ranged on a 4-point Likert scale from “absolutely agree/can” to “dislike/disagree/nil.” Participant-centric and parent-centric versions of the questionnaire were prepared. The questions were the same except for the corresponding target audiences, e.g., “You” in the participant-centric version and “Your child” in the parent-centric version.
Statistical Analysis
All data collected on the first day of the courses were grouped together to form the “Before” group, and data collected at the 10th class were grouped to form the “After” group, regardless of the course type and the time joining the classes. Grouping data from music and arts courses together aims at increasing the statistical power which made the hypothesis tests more sensitive given the principles behind the courses (training modalities) were similar.
Demographic characteristics were calculated using Student’s T- test (for numeric variables) or the Chi-square test (for categorical variables) where appropriate. Functional assessments (power grip, lateral pinch, and tip pinch for both sides) recorded before and after courses were compared using an independent sample T-test. Results from questionnaires (BOT-2, Subjective Happiness Scale, WHO-5, and CFESI-2) were also compared. Responses of the course evaluation questionnaires from participants and parents were compared using Chi-square tests. Age-specific analysis comparing the CFESI-2 domain score before and after courses were followed. Receiver operating characteristic (ROC) curve analysis on different age cut-off values in the sensitivity testing approach was carried out to find out the age threshold on how well the CFESI-2 social domain performed. Sensitivity, Specificity, positive predictive value (PPV), negative predictive value (NPV), the area under the curve (AUC), standard error (SE), and p values were tabulated by cut-offs. Data analysis was carried out using IBM SPSS 26.0 (Armonk, New York). A two-sided p value ≤ 0.05 was considered statistically significant.
RESULTS
Over the 3 years since the program launched, 35 participants (male = 20, female = 15) suffering from different kinds of abnormalities were recruited and participated a total of 152 course sessions. Mean age at recruitment was 8.65 ± 2.45 (range = 5.83, 16.75), with median = 8.53 (range = 6.98, 9.54). Four of them had left dominant hand and 14 had affected hand on the left side.
Types of Abnormalities
Major abnormalities and numbers of participants involved were described as follows: (a) 9 participants suffered from syndactyly, polydactyly, extra- or short-finger, (b) 13 suffered from muscular abnormalities, e.g., Myasthenia Gravis, muscular dystrophy, (c) 6 suffered from congenital deficiencies or disorders, e.g., ADHD, ASD, cretinism, dwarfism, epilepsy, mucopolysaccharidoses, and (d) others, e.g., burn or infection at fingers in 7 participants.
Functional Assessments and Outcomes of Psychosocial Centric Questionnaires
Functional assessments and questionnaire outcome scores collected before and after interest courses were compared (Table 1). The basic characteristics of the participants were quite similar to each other and so as the functional abilities when they first joined the courses. All comparisons in both functional assessments and psychosocial centric questionnaire outcomes did not show any statistical difference after joining the interest courses. Culture-free Self-esteem Inventory-2 social domain was worth exploring given the lowest p values among the comparisons (Table 1).
| Assessments | Before | After | p value |
|---|---|---|---|
| Function assessments | |||
| Power grip (left) | 6.44 | 7.04 | 0.572 |
| Power grip (right) | 6.58 | 6.84 | 0.774 |
| Lateral pinch (left) | 3.62 | 3.66 | 0.884 |
| Lateral pinch (right) | 3.64 | 3.66 | 0.907 |
| Tip pinch (left) | 3.13 | 3.34 | 0.450 |
| Tip pinch (right) | 3.02 | 3.45 | 0.378 |
| Questionnaires | |||
| BOT2 total | 25.61 | 26.13 | 0.658 |
| BOT2 scale mean score | 14.55 | 14.32 | 0.811 |
| Subjective happiness scale | 19.45 | 19.49 | 0.973 |
| WHO-5 score | 16.31 | 16.48 | 0.890 |
| WHO-5 score (in percentage) | 63.56 | 64.20 | 0.900 |
| CFESI-2 domains | |||
| General | 12.60 | 12.63 | 0.959 |
| Social | 5.35 | 5.81 | 0.170 |
| Academic | 6.35 | 6.44 | 0.816 |
| Parental | 7.63 | 7.37 | 0.577 |
| Total | 32.02 | 32.35 | 0.839 |
Cutoff Values of Age in Terms of CFESI-2 and ROC Sensitivity Analyses
Culture-free Self-esteem Inventory-2 social domain scores were stratified by 5 age-cut off points with reference to the median age (Table 2). Culture-free Self-esteem Inventory-2 social domain was significantly increased at age ≤7.5 (p = 0.01), age ≤8.5 (p = 0.03), and age ≤10.5 (p = 0.04). Receiver operating characteristic curve analyses followed, and the results were tabulated in Table 3. The AUC showed largest when the age cut-off was at 10.5, with statistical significance (p < 0.01). Receiver operating characteristic curves and AUC were plotted and shown in Figures 1 23.
| Age | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≤6.5 | >6.5 | ≤7.5 | >7.5 | ≤8.5 | >8.5 | ≤9.5 | >9.5 | ≤10.5 | >10.5 | ≤11.5 | >11.5 | |||||||||||||
| CFESI domains | Before | After | Before | After | Before | After | Before | After | Before | After | Before | After | Before | After | Before | After | Before | After | Before | After | Before | After | Before | After |
| General | 13.29 | 15.20 | 12.49 | 12.39 | 12.92 | 13.45 | 12.50 | 12.45 | 11.76 | 12.11 | 13.37 | 13.00 | 11.57 | 11.48 | 14.71 | 14.50 | 11.78 | 11.68 | 15.33 | 14.65 | 12.26 | 12.17 | 14.22 | 14.70 |
| Social | 5.14 | 6.40 | 5.38 | 5.78 | 5.00* | 6.73* | 5.45 | 5.60 | 4.92* | 5.89* | 5.74 | 5.81 | 5.06 | 5.61 | 5.94 | 6.20 | 4.88* | 5.62* | 6.92 | 6.29 | 5.14 | 5.71 | 6.33 | 6.40 |
| Academic | 5.86 | 7.40 | 6.42 | 6.37 | 5.67 | 7.00 | 6.55 | 6.33 | 6.08 | 6.26 | 6.59 | 6.59 | 6.03 | 5.97 | 7.00 | 7.25 | 6.08 | 6.03 | 7.25 | 7.35 | 6.16 | 6.20 | 7.22 | 7.60 |
| Parental | 8.00 | 8.60 | 7.58 | 7.23 | 8.00 | 8.36 | 7.53 | 7.10 | 7.32 | 7.68 | 7.93 | 7.18 | 7.20 | 6.69 | 8.53 | 8.45 | 7.30 | 6.83 | 8.75 | 8.47 | 7.37 | 6.93 | 8.89 | 9.20 |
| Total | 32.29 | 37.60 | 31.98 | 31.78 | 31.58 | 35.55 | 32.15 | 31.48 | 30.21 | 32.22 | 33.63 | 32.42 | 29.94 | 29.74 | 36.18 | 36.40 | 30.10 | 30.15 | 38.25 | 36.76 | 31.02 | 31.00 | 36.67 | 37.90 |
*p < 0.01
| ROC values | Age cutoff values | |||||
|---|---|---|---|---|---|---|
| 6.5 | 7.5 | 8.5 | 9.5 | 10.5 | 11.5 | |
| Sensitivity | 0.892 | 0.797 | 0.690 | 0.284 | 0.203 | 0.149 |
| Specificity | 0.862 | 0.724 | 0.473 | 0.552 | 0.517 | 0.724 |
| PPV | 0.725 | 0.738 | 0.339 | 0.568 | 0.517 | 0.579 |
| NPV | 0.333 | 0.348 | 0.795 | 0.197 | 0.203 | 0.250 |
| AUC | 0.469(0.301,0.637) | 0.446(0.313,0.580) | 0.576 (0.465, 0.686) | 0.621(0.502,0.740) | 0.700(0.586,0.814) | 0.652 (0.522, 0.781) |
| SE | 0.086 | 0.068 | 0.056 | 0.061 | 0.058 | 0.066 |
| p value | 0.731 | 0.435 | 0.190 | 0.042 | 0.002 | 0.040 |
PPV, positive predictive value; NPV, negative predictive value; AUC, area under curve; SE, standard error
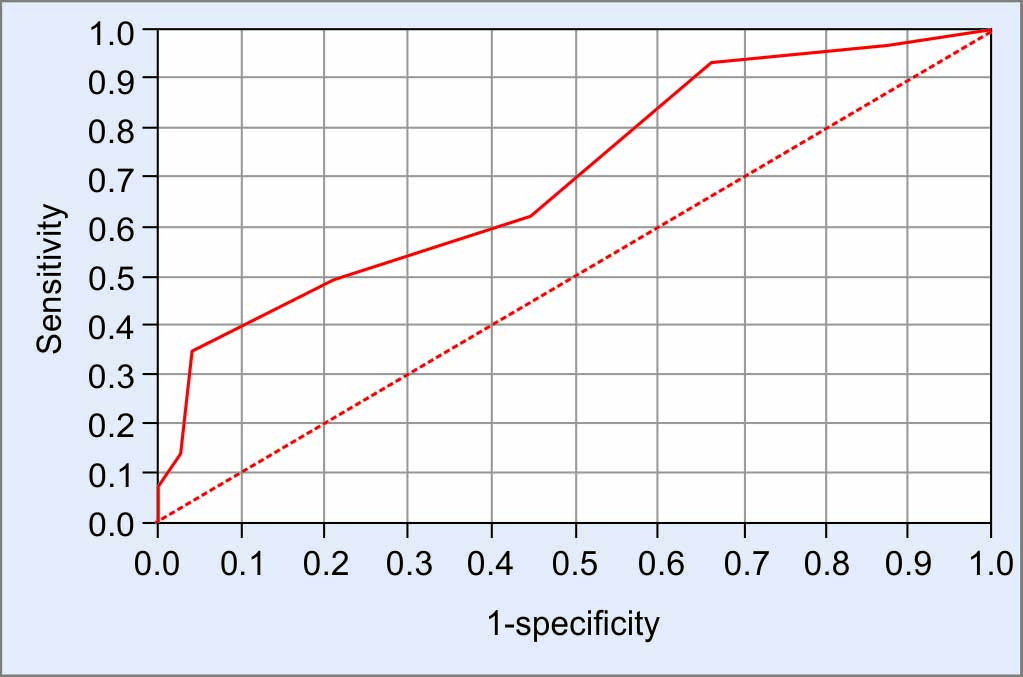
Fig. 1: ROC curve of CFESI-2 social domain when age = 10.5

Fig. 2: ROC curve of CFESI-2 social domain when age = 9.5
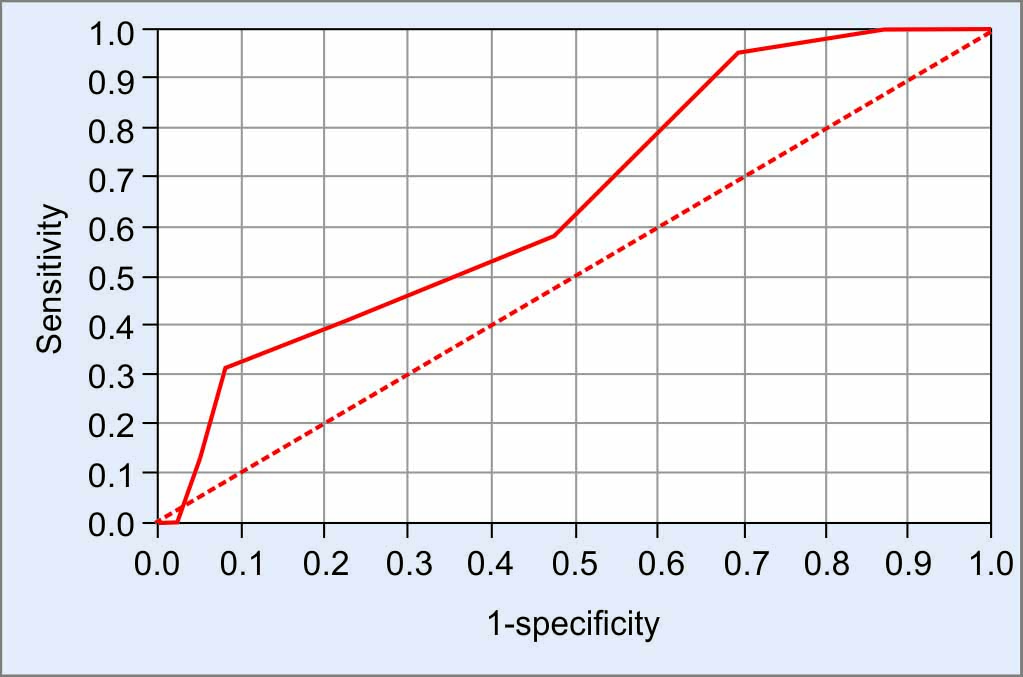
Fig. 3: ROC curve of CFESI-2 social domain when age = 11.5
Course Evaluation Questionnaire
Overall speaking, both participants and parents favorably responded after the courses (Table 4). Participants and parents felt “much like” or “like” to the course (86.9 and 89.7%), more willing to use hands (75.3 and 90.7%), improved social activities (79.7 and 94.4%), hand function (72.4 and 92.5%), and self-confidence (78.2 and 87.1%). Parents agreed that hand function was a significant improvement after completing the 10 classes (44.4 vs 24.6%, p = 0.01).
| Questions | Participants | Parents | p value |
|---|---|---|---|
| Question 1: What do you feel about “Budding Well” program | |||
| Much like | 35 (49.3) (50.7) | 36 (50.7) (66.7) | 0.17 |
| Like | 25 (61.0) (36.2) | 16 (39.0) (29.6) | |
| Neither like nor dislike | 7 (77.8) (10.1) | 2 (22.2) (3.7) | |
| Dislike | 2 (100.0) (2.9) | 0 (0.0) (0.0) | |
| Question 2: Do you think you/your child is more willing to use their hands to handle daily activities after coming through the “Budding Well” program? | |||
| Many times | 35 (53.0) (50.7) | 31 (47.0) (57.4) | 0.12 |
| Sometimes | 17 (48.6) (24.6) | 18 (51.4) (33.3) | |
| As normal | 14 (73.7) (20.3) | 5 (26.3) (9.3) | |
| Nil | 3 (100.0) (4.3) | 0 (0.0) (0.0) | |
| Question 3: Do you think you/your child is more willing to participate in different social activities after coming through the “Budding Well” program? | |||
| Absolutely agree | 29 (49.2) (42.0) | 30 (50.8) (55.6) | 0.11 |
| Agree | 26 (55.3) (37.7) | 21 (44.7) (38.9) | |
| Neither agree nor disagree | 13 (81.3) (18.8) | 3 (18.8) (5.6) | |
| Disagree | 1 (100.0) (0.0) | 0 (0.0) (0.0) | |
| Question 4: Does your/your child’s hand function improve after coming through the “Budding Well” program? | |||
| Absolutely agree | 33 (55.9) (47.8) | 26 (44.1) (48.1) | 0.01 |
| Agree | 17 (41.5) (24.6) | 24 (58.5) (44.4) | |
| Neither agree nor disagree | 15 (78.9) (21.7) | 4 (21.1) (7.4) | |
| Nil | 4 (100.0) (0.0) | 0 (0.0) (0.0) | |
| Question 5: Does your/your child’s self-confidence improve after coming through the “Budding Well” program? | |||
| Absolutely can | 29 (50.9) (42.0) | 28 (49.1) (51.9) | 0.34 |
| Can | 25 (56.8) (36.2) | 19 (43.2) (35.2) | |
| A little bit | 12 (63.2) (17.4) | 7 (36.8) (13.0) | |
| Cannot | 3 (100.0) (4.3) | 0 (0.0) (0.0) | |
DISCUSSION
Harmonica play and drawing courses are two purposeful activities that our participants actively attended with great interests. Different from the routinized therapy modalities in standard rehabilitation procedures, participants can gain therapeutic values using musical and colorful instruments with intense enjoyment. Advantages coming through harmonica playing and drawing require competent manual dexterity, limb abilities of the participants were therefore expected to improve through their weekly practice (training). Given the light weight of harmonica itself or drawing instruments not serving a weight-lifting purpose on muscle training, no statistical significance (improvement) was found in participants’ functional grip and pinch strength, as well as their dexterity skills after the interest courses.
The difference between the pre- and posttests of the subjective happiness scale and the WHO-5 on subjective well- being was not significant. Sample size could be one of the limiting factors. High adaptability of the participants to their physical conditions was speculated being a response on the already restored competence, including the skills demanded coping with the harmonica itself and drawing equipment. The high physical condition adaptability through living demands make the happiness and mental well-being gains after completing the interest courses invisible. Social domain from CFESI-2 still demonstrates favorable results after the living adaption. Budding Well program proves to provide a strong positive engagement on interpersonal relationships in terms of self-esteem.
Self-esteem, donated by CFESI-2 Social domain, was significantly improved at age 10.5 through the results from ROC sensitivity analysis. Age is a major confounding factor of self-esteem (CFESI-2 Social domain) and this is overcome by stratifying the dataset by age groups. Self-esteem is shown to be age-dependent,18,19 and the reported age of awareness is 10 years old.20,21 Self-esteem is defined as a person’s subjective evaluation of his or her worth as a person. It is a subjective construct regardless of how others perceive the characteristics of the person.18 Our reported age of awareness (10.5 years old)20,21 matches Harter’s stipulation of the transition change from middle childhood to adolescence. A possible decline in self-esteem is observed due to the increasing emphasis on social comparison and pubertal changes.22,25 Study series from Harter focused on the development of self-esteem during childhood and adolescence.23 Regarding mean-level change, Harter identified several processes that marked the ups and downs in self-esteem from early to middle childhood (i.e., from about age 4–8 years). During early childhood, children are not yet able to distinguish between their actual and ideal competencies. When they learn to discriminate between their actual and ideal characteristics, this process leads to reduced positivity of self-descriptions. When they can use social comparison information in their self-evaluation at growing up, their self-esteem declines again when they overcome this cognitive limitation in middle childhood. A third social- cognitive process is perspective-taking. Children have considerably improved their social perspective-taking skills and self-esteem at age 8. Thus, beginning in middle childhood, children’s self-views are more strongly influenced by how others perceive them. However, children experience a decline in self-esteem during the transition to adolescence. The decline may become stronger while facing social comparison, less personal attention by teachers, and pubertal changes.22,25 Results from a meta-analysis showed that average levels of self-esteem increased from age 4 to 11 and remained stable from age 11 to 15.18 Positive self-esteem trajectory in childhood suggested a transition from early to middle childhood.26
Budding Well program chose music (harmonica playing) and arts (drawing) as teaching media. In the harmonica course, the use of harmonica was structured to involve all the sensory organs: the rhythmic and melodic components of music being specific stimuli to obtain certain motor and emotional responses. This was achieved by combining motor movement with multiple sensory stimulations with well-established emotional quality. Through active group music intervention, participants’ motivation and life force are enhanced through classical biophysiological responses such as movement and emotional catharsis, as well as through self- discovery and awareness, and increased self-esteem and pleasure.26 In drawing course, accomplishment is reached accompanying teachers, group mates, parents, and most importantly–the participants themselves. They have been rewarded by the visual gift created by themselves. They learn to make decisions on choosing the colors and shapes, enhancing their abilities to direct behavior, making choices, and risks. The artwork is unique and shows the “can do” spirit. The participants validate themselves and empower their uniqueness, therefore, enhance their sense of self- worth and self-esteem.27 Through group play, participants learn how they can reach good performances. Cooperative group work can be praised by teachers and group mates, leading to positive perceptions from the others and their parents. They learn how to work with others, and this will further consolidate the inter-personal relationships among this specific kind of participants and other people in the society. With reference to the favorable opinions (perception on hand function) from both participants and parents after coming through the program, the following further studies are recommended. Outcomes of functional grip, pinch strength, and dexterity skills can be further evaluated under a long-term longitudinal follow-up study design. Increasing the sample size can improve the data generalizability, and therefore can review the subjective happiness scale and well-being scales again. Moreover, a long-term follow-up of these kinds of patients monitors the time- dependent functional and psycho-sociological changes.
Limitations
A small sample size of this study limits the data generalizability, despite this is inevitable under limited resources and a limited number of teachers provided. Individual differences in abilities are fundamental and inevitable. These differences are not accountable to the effectiveness of the interest courses. We admitted that the variety of patients involved was broad. This was a rehabilitation service for these unfortunate children. The initial design and data quality in terms of the kinds of data collected kept the service running smoothly. Data collection might not be totally transferrable to carry out suitable statistical analysis. This article reported the overview of the rehabilitation program and functional outcomes after the program for these unfortunate children. Further analysis by dividing the children into congenital, injury, and neuromuscular groups would be appreciated. Moreover, the reasons for improving the hand grip scores might not be solely influenced by the program, e.g., the children were growing over time. Individual responses after the interest courses are largely different from each other and are possibly independent of the underlying principle and design of the program. The placebo effect might affect the results from course evaluation questionnaires from both participants and parents.
CONCLUSION
Hand functions and psychosocial skills of children and teenagers with different levels of physical disabilities or disfigurement proved to be beneficial from our program composing of music and art interest classes. Participants of age at 10.5 best responded to the program, particularly on the significant improvement in self- esteem. Long-term follow-up on these patients was recommended to look for the longitudinal changes of their functional impairments at their upper and/or lower limbs.
PATIENT DECLARATION STATEMENT
“The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/ their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.”
ACKNOWLEDGMENTS
SK Yee Medical Foundation, Hong Kong Harmonica Association, Art in Hospital, Slix Society, Department of Orthopaedics and
Traumatology, Prince of Wales Hospital, Hong Kong SAR, Prosthetics and Orthosis department, Prince of Wales Hospital, Hong Kong SAR, Health Resource Centre, Prince of Wales Hospital, Hong Kong SAR, Department of Rehabilitation Sciences, Hong Kong Polytechnic University, HKU School of Professional and Continuing Education, HK Burns Association.
REFERENCES
1. Budding_Well. [Budding Well]. Available at: https://www.facebook.com/buddingwell/.
2. Bruininks RH. Bruininks-Oseretsky test of motor proficiency: examiner’s manualed. American Guidance Service; 1978.
3. Bruininks RH, Bruininks BD. BOT2: Bruininks-Oseretsky test of motor proficiency: manualed. Pearson Assessments; 2005.
4. Deitz JC, Kartin D, Kopp K. Review of the Bruininks-Oseretsky test of motor proficiency. 2nd ed. (BOT-2). Phys Occupat Therapy Pediat 2007;27(04):87–102. DOI: 10.1080/J006v27n04_06
5. McQuiddy VA, Scheerer CR, Lavalley R, et al. Normative values for grip and pinch strength for 6- to 19-year-olds. Arch Phys Med Rehabil 2015;96(09):1627–1633. DOI: 10.1016/j.apmr.2015.03.018.
6. Bohannon RW. Hand-grip dynamometry provides a valid indication of upper extremity strength impairment in home care patients. J Hand Ther 1998;11(04):258–260. DOI: 10.1016/s0894-1130(98)80021-5
7. Molenaar HM, Zuidam JM, Selles RW, et al. Age-specific reliability of two grip-strength dynamometers when used by children. J Bone Joint Surg Am 2008;90(05):1053–1059. DOI: 10.2106/JBJS.G.00469
8. Peolsson A, Hedlund R, Oberg B. Intra- and inter-tester reliability and reference values for hand strength. J Rehabil Med 2001;33(01):36–41. DOI: 10.1080/165019701300006524
9. Bellace JV, Healy D, Besser MP, et al. Validity of the Dexter evaluation system’s Jamar dynamometer attachment for assessment of hand grip strength in a normal population. J Hand Ther 2000;13(01):46–51. DOI: 10.1016/s0894-1130(00)80052-6
10. Mathiowetz V. Comparison of Rolyan and Jamar dynamometers for measuring grip strength. Occup Ther Int 2002;9(03):201–209. DOI: 10.1002/oti.165
11. Shechtman O, MacKinnon L, Locklear C. Using the BTE Primus to measure grip and wrist flexion strength in physically active wheelchair users: an exploratory study. Am J Occup Ther 2001;55(04):393–400. DOI: 10.5014/ajot.55.4.393
12. King TI. Interinstrument reliability of the Jamar electronic dynamometer and pinch gauge compared with the Jamar hydraulic dynamometer and B&L engineering mechanical pinch gauge. Am J Occup Ther 2013;67(04):480–483. DOI: 10.5014/ajot.2013.007351
13. Mathiowetz V, Weber K, Volland G, et al. Reliability and validity of grip and pinch strength evaluations J Hand Surg Am 1984;9(02):222–226. DOI: 10.1016/s0363-5023(84)80146-x
14. Lyubomirsky S, Lepper HS. A measure of subjective happiness: preliminary reliability and construct validation. Soc Indicat Res 1999;46(02):137–155. DOI: 10.1023/A:1006824100041
15. Nan H, Ni MY, Lee PH, et al. Psychometric evaluation of the Chinese version of the subjective happiness scale: evidence from the Hong Kong FAMILY Cohort. Int J Behav Med 2014;21(04):646–652. DOI: 10.1007/s12529-014-9389-3
16. Topp CW, Østergaard SD, Søndergaard S, et al. The WHO-5 Well- Being index: a systematic review of the literature. Psychother Psycho 2015;84(03):167–176. DOI: 10.1159/000376585
17. Chan Y-HY, The normative data and factor structure of the culture- free self-esteem inventory-form a-second edition in Hong Kong adolescents. HKU Theses Online (HKUTO): The University of Hong Kong (Pokfulam, Hong Kong), 2002.
18. Orth U, Erol RY, Luciano EC. Development of self-esteem from age 4 to 94 years: A meta-analysis of longitudinal studies. Psychol Bull 2018;144(10):1045–1080. DOI: 10.1037/bul0000161
19. Orth U. The family environment in early childhood has a long-term effect on self-esteem: a longitudinal study from birth to age 27 years. J Personal Soc Psychol 2018;114(04):637–655. DOI: 10.1037/pspp0000143
20. Daniels DH. Age differences in concepts of self-esteem. Merrill Palmer Q 1998;44:234–258.
21. Helwig N, Ruprecht M. Age, gender, and self-esteem: a sociocultural look through a nonparametric lens. Archi Scienti Psychol 2017;5(01):19–31. DOI: 10.1037/arc0000032
22. Harter S. Developmental and individual difference perspectives on self-esteem. Handbook of personality development. Mahwah, NJ, US: Lawrence Erlbaum Associates Publishers; 2006. pp. 311–334.
23. Harter S. The development of self-esteem. Self-esteem issues and answers: a sourcebook of current perspectives. New York, NY, US: Psychology Press; 2006. pp. 144–150.
24. Harter S. The self. Handbook of child psychology: social, emotional, and personality development, vol. 3 6th ed., Hoboken, NJ, US: John Wiley & Sons Inc; 2006. pp. 505–570.
25. Harter S. The construction of the self: developmental and sociocultural foundations. In: The inextricable link between perceived physical appearance and self-esteem. Ch. 5, 2nd ed., New York, NY, US: Guilford Press; 2012. pp. 158–193.
26. Choi AN, Lee MS, Lee JS. Group Music Intervention Reduces Aggression and Improves Self-esteem in Children with Highly Aggressive Behavior: A Pilot Controlled Trial. Evid Based Complement Alternat Med 2010;7(02):213–217. DOI: 10.1093/ecam/nem182
27. Mak HW, Fancourt D. Arts engagement and self-esteem in children: results from a propensity score matching analysis. Ann New York Acad Sci 2019;1449(01):36–45. DOI: 10.1111/nyas.14056
________________________
© The Author(s). 2022 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.