CASE REPORT | https://doi.org/10.5005/jp-journals-10079-1006 |
Double Patella Syndrome Following Hoffa’s Fat Pad Lesion
1–3Department of Orthopaedics, Devadoss Hospitals Pvt Ltd, Madurai, Tamil Nadu, India
4Department of Orthopaedics and Spine, Devadoss Multispeciality Hospital, Madurai, Tamil Nadu, India
Corresponding Author: Annamalai Devadoss, Department of Orthopaedics, Devadoss Hospitals Pvt Ltd, Madurai, Tamil Nadu, India, Phone: +91 9790034358, e-mail: profdevadoss@gmail.com
How to cite this article Aakash K, Devadoss A, Devadoss S, et al. Double Patella Syndrome Following Hoffa’s Fat Pad Lesion. J Orth Joint Surg 2019;1(1):35–37.
Source of support: Nil
Conflict of interest: None
ABSTRACT
Patellar duplication is a rare asymptomatic condition. The diagnosis is often made following a traumatic event associated with an injury to the knee extensor mechanism. The treatment is often surgical and consists of removal of the smaller part of the patella with tendon reinsertion; the case presented here did not have a sleeve avulsion fracture of patella but still developed a osseous lesion resembling patella. The possible theory for this finding could be due to a hematoma formation in Hoffa’s fat pad that could have been calcified, then later ossified. This case is being report due to its rare occurrence.
Keywords: Double patella, Extensor mechanism of knee, Hoffa’s fat pad lesion, Patella duplication.
BACKGROUND
Duplication of the patella is rare occurrence. Since the first case was described, very few have been reported till now. Double patella was first described by Trillat,1 as an uncommon clinical feature following repetitive injuries of the extensor mechanism of the knee, and the first injury is a tendoperiosteal avulsion of the suprapatellar or less frequently, infrapatellar tendon from the corresponding patellar pole. Often, these avulsions are misdiagnosed and therefore treated only with a cast or no immobilization at all. The causes for the double patella reported in the literature are usually traumatic and congenital, and few cases have been reported to be associated with epiphyseal dysplasia.2,3 In our case, though the patient had a history of trauma, there was no associated fracture of patella. The possible theory for this finding could be due to a hematoma formation in Hoffa’s fat pad that could have been calcified, then later ossified. This case is being report due to its rare occurrence.
CASE DESCRIPTION
A 47-year-old male patient presented to us with the complaints of right knee pain for 5 years. He had a history of trivial trauma to right knee following a fall 5 years back, but he was able to walk immediately following fall and did not seek any medical attention at the time of fall. He developed restriction of knee flexion for 3 years and has difficulty in squatting and running. There was no history of giving away and locking episodes of affected knee. On examination, supra and infra patellar swelling was noted (Fig. 1), and bony hard mass was felt on the infra patellar region with palpable gap between patella and the infra-patellar mass. The mass was slightly mobile and was nontender. There was no effusion of the joint. Knee instability tests were normal, range of motion of right knee was 0°–90°, and beyond 90° flexion was restricted (Fig. 2). Radiographic examination showed circumscribed bony mass below the patella (Fig. 3). Computed tomography (CT) and magnetic resonance imaging (MRI) showed circumscribed mass of size 3.5 × 2.2 cm situated inferior to patella over Hoffa’s fat pad, patellar tendon was found to be intact (Fig. 4). Surgical management in the form of excision of the mass was planned.
Surgery was performed under spinal anesthesia, under tourniquet control with the patient in supine position. The approach was through a midline skin incision made over the right knee, and the knee joint was exposed through a medial parapatellar approach. An ossified mass was found medial to patellar tendon without any attachments to underlying structures, and patella tendon was found intact (Fig. 5) with Insall index of 1:1. Hence, plication was not required. Following excision of the mass, a full range of knee flexion was achieved intraoperatively. Macroscopically, the excised mass resembled patella anatomically, and it was irregularly distributed with cartilage (Fig. 6). Cut sections showed bony trabeculae, and the specimen was sent for histo-pathological examination. Histopathological examination (HPE) showed mature bony tissue with cartilage.

Fig. 1: Right knee showing infrapatellar mass

Figs 2A and B: Flexion of right knee restricted to 90°
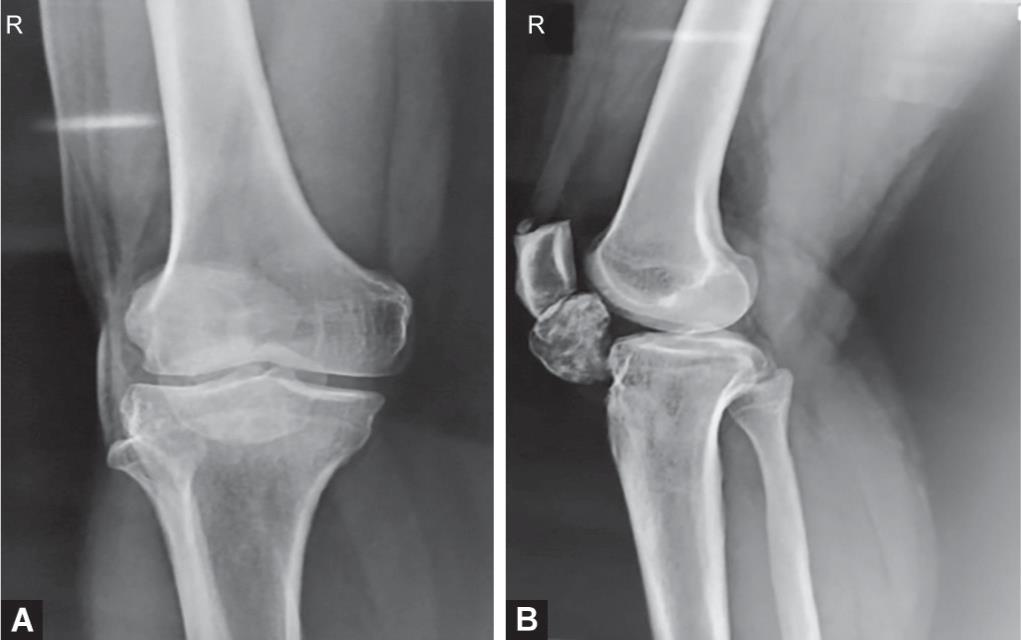
Figs 3A and B: Preoperative X-ray of right knee showing infrapatellar bony mass

Figs 4A and B: (A) Preoperative CT scan; (B) MRI showed bony mass of size 3.5 × 2.2 cm

Figs 5A and B: Intraoperative images after excision showed mass similar to patella

Fig. 6: Cut section of mass showed bony trabeculae
The immediate postoperative X-ray after removal of the bony mass has been shown in Figure 7. Postoperatively, knee range of movements was started from day 2 to prevent knee stiffness, Isometric quadriceps exercises were initiated immediately after surgery. He was discharged on the 5th postoperative day. Sutures were removed on the 12th postoperative day. At 4 weeks follow-up, the patient had a full range of movements without extension lag (Fig. 8).
DISCUSSION
Two etiological theories explain the development of a duplicate patella. The first hypothesis refers to a congenital malformation. This assertion is supported by the report of bilateral horizontal cases,3 and the observation of coronal4 and frontal patellar duplication (also called double layer patella, reported in patients with multiple epiphyseal dysplasia).2,5 A fully developed tendon between the two patellar parts was described in these reports.
The second hypothesis considers the duplicate patella as the result of the natural healing of an undiagnosed sleeve fracture. This fracture occurs in skeletally immature patients and represents a traumatic avulsion of the extensor mechanism with a small sleeve of cartilage and periosteum. These fractures can occur at either the proximal or the distal pole of the patella. The treatment is mainly surgical; however, some cases were successfully treated with braces.1 The osteogenic potential of the cartilage sleeve explains the evolution toward a duplicate patella.6,7
The case presented here did not have a sleeve avulsion fracture of patella, and the excised mass was resembling the exact shape and size of an original patella as shown in the images above. A duplicate patella is not commonly related to patients with Hoffa’s fat pad hematoma from any cause, and we were unable to find other reported cases in the literature with this kind of association. The duplicate patella’s etiology remains unclear. The hematoma formation in Hoffa’s fat pad could have been calcified and then later ossified. We are reporting this case for its rarity. In our case, the extensor mechanism was totally spared and after excision of the mass, the patella tendon was found to be intact with Insall index of 1:1 ratio. The patient achieved full knee flexion after the surgical excision and has excellent outcome during further follow-ups.

Figs 7A and B: Postoperative X-ray of right knee after mass excision

Fig. 8: Patient had a full range of knee flexion at 1 month follow-up
CONCLUSION
Double patella syndrome is rare clinical condition and often misdiagnosed and often untreated, and Hoffa’s fat pad lesion should also be considered in development of an osseous lesion in the suspected cases.
REFERENCES
1. Trillat A. Chirurgie du genu. Lyon: Simep Editeur; 1976.
2. Yochum TR, Sprowl CG, Barry MS. Double patella syndrome with a form of multiple epiphyseal dysplasia. J Manipulative Physiol Ther 1995;18(6):407–410.
3. Grogan DP, Carey TP, Leffers D, et al. Avulsion fractures of the patella. J Pediatr Orthop 1990;10(6):721–730. DOI: 10.1097/01241398-199011000-00004.
4. Gasco J, Del Pino JM, Gomar-Sancho F. Double patella. A case of duplication in the coronal plane. J Bone Joint Surg Br 1987;69(4):602–603. DOI: 10.1302/0301-620X.69B4.3611165.
5. Hodkinson HM. Double patellae in multiple epiphysial dysplasia. J Bone Joint Surg Br 1962;44-B:569–572.
6. Houghton GR, Ackroyd CE. Sleeve fractures of the patella in children: a report of three cases. J Bone Joint Surg Br 1979;61-B(2):165–168.
7. Yeung E, Ireland J. An unusual double patella: a case report. Knee 2004;11(2):129–131. DOI: 10.1016/S0968-0160(03)00040-1.
________________________
© The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.